Written by: Brian Cole
By early March, it was becoming increasingly clear that the novel coronavirus that causes COVID-19 would not be contained.
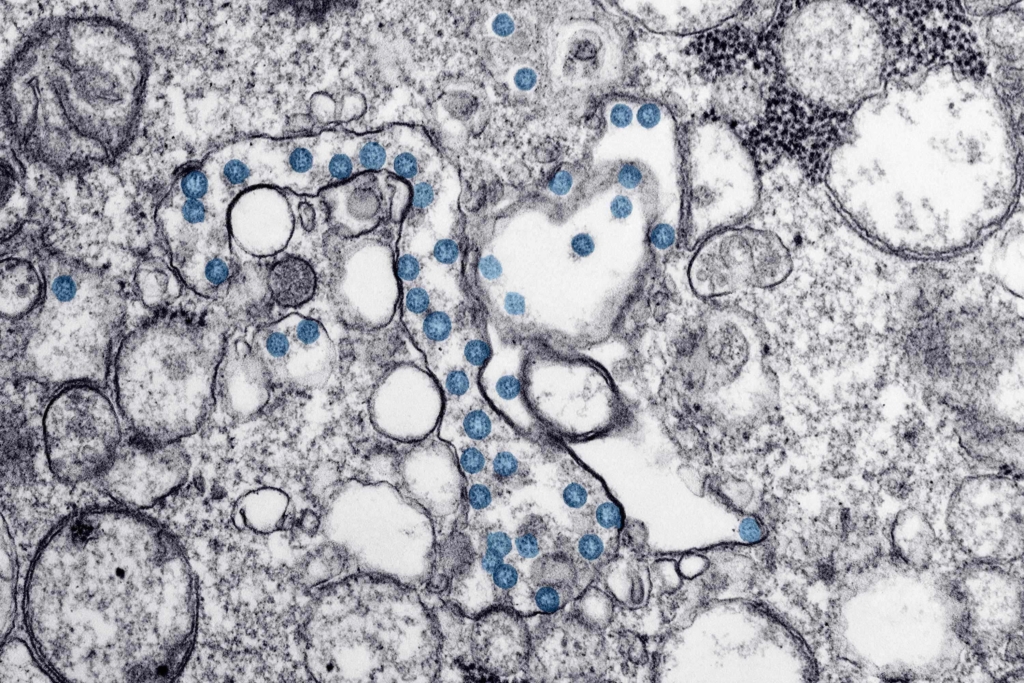
Just a few months earlier, the virus – officially known as severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2 – had emerged in Wuhan, China, prompting a lockdown of more than 11 million people in that city.
Now it was moving across Asia, into Europe and North America, killing hundreds of people and infecting thousands more. Suddenly, a virus once assumed to be under control was well on its way to becoming the deadliest global pandemic since the Spanish Flu in 1918, which killed an estimated 50 million people around the world.
By this time, Dr. Ryan Zarychanski had already started to take note.
A hematologist, critical care physician and clinical scientist at CancerCare Manitoba and the University of Manitoba, Zarychanski heads up a team of researchers who normally spend their time investigating the effectiveness of therapies for various blood conditions in critically ill patients.
But these were not normal times. Zarychanski knew the virus would eventually find its way to Manitoba (the first cases were reported on March 12), and that hospitals here would have no specific therapies for those who became infected or who were at risk of contracting COVID-19.
“When COVID came around, it was apparent very quickly that there were no proven therapies (to treat patients),” says Zarychanski. “All we could offer patients was supportive care – a hospital bed, supplemental oxygen, symptom control, organ support should they become critically ill, and managing complications caused by the virus.”
He also knew there was only one way to solve that problem: clinician-scientists in Manitoba would have to join the world-wide effort to test the effectiveness of experimental therapies in scientifically rigorous clinical trials.
Fortunately, Zarychanski’s team had the knowledge and experience to do just that.

Normally, the acute care hematology research team has about 14 members, including physicians, nurses and trainees. While most members of his team are working on clinical trials for COVID-19, Zarychanski still had to expand the team by as many as 18 additional researchers, including research co-ordinators, investigators, infectious disease physicians, nurses and medical students, to carry out the work. The expanded team has set to work activating or developing COVID-19 clinical trials across the entire spectrum of disease severity. All told, the team has launched, or are about to launch, no less than eight clinical trials involving six different therapies. They include:
* Hydroxychloroquine. This drug, which is commonly used to treat autoimmune conditions such as lupus and rheumatoid arthritis, or to prevent or treat malaria, was used in three trials in Manitoba involving people who have COVID-19, family members who are living with someone who has the disease, and health-care workers who were exposed to patients with COVID-19.
* Heparin. This drug is a blood thinner used to treat and prevent blood clots, but also has anti-inflammatory effects and may have specific anti-viral properties. Heparin is being given to patients in two trials, including those admitted to a hospital ward and those being treated in an intensive care unit.
* Interferon beta-1a. This drug, which is used to treat patients with multiple sclerosis, has anti-viral properties and plays a role in regulating the immune response. It is being used in one clinical trial in Manitoba involving patients who have been admitted to an intensive care unit.
* Lopinavir/ritonavir. Used to treat patients with HIV infection, this drug will be used in one upcoming clinical trial involving patients who are admitted to a hospital ward and those being treated in an intensive care unit.
* Remdesivir. This is an anti-viral medication that has been used in patients with SARS-CoV (severe acute respiratory syndrome coronavirus) and the Middle East respiratory syndrome (MERS-CoV). Once the trial is underway, the drug will be given to patients who are admitted to a hospital ward and those being treated in an intensive care unit.
* Convalescent plasma. This therapy involves collecting plasma from people who have recovered from COVID-19 and giving it to patients who are sick with the disease. The idea is that the blood from people who have recovered from the disease will have antibodies that can help the recipient patient fight off the virus. One trial involving hospital ward patients is currently open and enrolling patients across Canada. A second trial, involving intensive care unit patients, is expected to start shortly.
Each of the clinical trials are designed to determine whether a particular therapy can help improve clinical outcomes in patients with COIVD-19, or prevent infection in those exposed to the virus. Although the number of Manitobans infected with COVID-19 has declined markedly in the last month or two (from 163 active cases in early April to 17 as of June 29), dozens of local patients have participated in the trials so far.
“Exceptionally long days have been required to action and organize these trials. All members of the team have been working flat-out so that Manitobans can have access to treatments in the context of high-quality and appropriately monitored clinical trials.”
Of all the therapies being reviewed, it is hydroxychloroquine that has garnered the most media attention. As readers may recall, the drug had been touted early on as a potential “game changer” by United States President Donald Trump.
But controversy ensued when the World Health Organization announced in late May that it was suspending clinical trials involving 3,500 patients in 17 countries following a report that COVID-19 patients receiving hydroxychloroquine were dying at a faster rate than those who did not receive the drug. That decision was based on an observational study, as opposed to a more scientifically rigorous randomized trial. More recently, the observational study has been withdrawn and the WHO has lifted the suspension.
Meantime, Zarychanski says one hydroxychloroquine study that Manitoba helped lead in Canada has been completed, with results published earlier this month in the New England Journal of Medicine. The study found that the drug had no real ability to prevent COVID-19 infection in those with high-risk exposures to COVID-19.
“The incidence of new symptoms compatible with COVID-19 did not differ significantly between participants receiving hydroxychloroquine or those receiving placebo,” the study says. “Side effects were more common with hydroxychloroquine than with placebo, but no serious adverse reactions were reported.”
Zarychanski says a second hydroxychloroquine study for hospitalized patients is still ongoing in Manitoba as part of a larger global trial. Preliminary results from observational studies are not uniformly encouraging.
“My thought at this point is that there might be too much emphasis here on one drug (hydroxychloroquine)” says Zarychanski. “We have no less than five other trials ongoing that are evaluating promising and exciting agents. It would be a lost opportunity to focus only on this one drug.”
As it turns out, one of the more promising therapies under review involves heparin, which is the subject of two international studies being led by Zarychanski’s team.
Zarychanski has spent several years studying the efficacy of heparin in reducing inflammation and blood clots in people with life threatening infection. So, when it became clear COVID-19 was associated with inflammation and blood clots, many of Zarychanski’s colleagues in the scientific community asked if he would be willing to head up an international study on the drug.
“After receiving daily e-mails from physicians around the world, it became obvious that I was going to have to help organize a large international randomized trial to figure out if heparin is beneficial for patients with COVID-19” says Zarychanski. “So, we rolled up our sleeves and got to work developing and launching such a trial.”
“People have just come together to make these trials a success. Research Manitoba should be acknowledged as a big part of that early success. Start-up funds were critical to the earlier initiation of the trials in Manitoba and to attract international engagement for the trials led in our province.”
The Manitoba-led trial was launched on May 12, with the enrolment of a patient from a Chicago hospital. The trial will include patients from hospitals in Canada, the U.S., Brazil, and Mexico. It is expected hospitals in the United Kingdom and the European Union will begin enrolling patients in the trial in the near future.
Although it is impossible to predict the study’s outcome, there is good reason to think that heparin may prove useful in treating COVID-19, partly because of the way the infection attacks the body.
As Zarychanski explains, early reports often attributed COVID-19 deaths to respiratory problems, such as pneumonia. But deaths are also caused by a variety of other health problems, including, heart attack, stroke and kidney failure.
“Almost everyone (who dies from COVID-19) dies ultimately from organ failure,” says Zarychanski. “The predominant organ failure starts as respiratory (lung) failure. But as you get sicker, other organs fail,” he says.
Multiple organ failure can be attributed to wide-spread inflammation, which is caused in part by blood clots. “Those processes are tightly linked. Clots lead to inflammation and inflammation leads to clots. All of that conspires to cause organ failure and death.”
Heparin might help break the cycle.
“Heparin is a blood thinner that also has anti-inflammatory properties and may have specific anti-viral properties as well,” says Zarychanski. “Heparin reduces blood clots, and if it reduces blood clots, it will probably reduce inflammation,” he says.
But the question that still has to be answered is: “If heparin reduces inflammation and blood clots, will it then prevent organ dysfunction and death in some patients?”
Zarychanski says he is proud of the way his team has been able to quickly pivot from their regular jobs to launch clinical trials for potential COVID-19 treatments.
“Exceptionally long days have been required to action and organize these trials” says Zarychanski. “All members of the team have been working flat-out so that Manitobans can have access to treatments in the context of high-quality and appropriately monitored clinical trials.”
Of course, none of it would have been possible without about $1.6 million in start-up support from the provincial government and Research Manitoba. The Manitoba Medical Services Foundation also provided funding to complete the first hydroxychloroquine trial. More recently, Zarychanski’s team has received $3.6 million and $2.2 million from the Canadian Institutes of Health Research to fund the heparin and convalescent plasma trials, respectively.
“People have just come together to make these trials a success,” says Zarychanski. “Research Manitoba should be acknowledged as a big part of that early success. Start-up funds were critical to the earlier initiation of the trials in Manitoba and to attract international engagement for the trials led in our province,” he says.
“Likewise, the institutional support of the University of Manitoba, CancerCare Manitoba, Shared Health and the Winnipeg Regional Health Authority, as well as direct support of the medical officers of health in Manitoba have been critical to the team’s success,” he says.
“I can’t stress enough how our phenomenally successful clinical trials response is due to the collective effort of many individuals and organizations in the province. This is a time to be proud of our province,” he says.
While launching a clinical trial to test the usefulness of a particular drug may sound fairly straightforward, organizing one is actually quite complicated, according to Nicole Marten, who is the senior research nurse and project co-ordinator on Zarychanski’s team.

As she explains, the process begins with an idea – a researcher develops a hypothesis that a particular treatment may be useful in treating a specific disease. The next step is to review the literature to determine if anyone else has done any research into the drug.
Once the literature review is complete, a researcher may connect with other investigators to see if there is any interest in collaborating on a clinical trial. That would be followed by the development of testing protocols, which would cover the type of drug, the dosage, and other particulars of the clinical trial including the type of clinical trial, sample size required, and budget needed to complete the trial.
“That protocol would then come to someone like me who would be responsible for submitting the proposal for approval to Health Canada, the Food and Drug Administration in the United States (or the appropriate regulatory body),” says Marten.
Young scientists get valuable experience
Once those approvals are acquired, the proposal is then forwarded for review to the appropriate local ethics committee, which could be a university or provincial body.
“Once Health Canada approves, and the local ethics committee and hospital approves, and once all the necessary legal contracts are in place, then you can start recruiting participants into the trial,” says Marten.
Needless to say, the process, which involves making sure all the steps are completed at every site participating in the trial, takes considerable time to finalize. Marten says some trials can take more than a year to get off the ground. However, because of the urgency surrounding COVID-19, Zarychanski’s team was able to get trials approved and launched in as little as six days.
“It’s been crazy fast,” she says. “And crazy exhausting.”
Part of the efficiency can be attributed to the “pandemic plan” for approving clinical trials that was put into place by Manitoba universities and hospitals following the H1N1 flu outbreak in 2009. “Because of H1N1, everyone asked, ‘How do we improve?’” says Marten.
Once a trial is up and running, research team members then focus on gathering data. Each trial will have its own dedicated team, including an investigator and a research co-ordinator. They are responsible for the day-to-day administration of therapies and making the sure the trial is being properly run according to national and international standards. The data from each trial is also reviewed by a panel of experts to ensure the study is being conducted safely.
Zarychanski says one of the remarkable things about the work being carried out on COVID-19 has been the degree of collaboration among research teams around the world.
“I’ve never witnessed this degree of collaboration before,” says Zarychanski. “We’re sharing processes, infrastructure, and ideas in ways that we’ve never thought to share.”
As a result, he says knowledge that would normally take years to generate has been pulled together in as little as two months. Zarychanski says he will not be surprised if researchers don’t start coming up with some potential treatments in the near future.
“We might not have a vaccine for a while, but I think the odds of having one or more useful treatments in the near future are very good.”
Brian Cole is a Winnipeg writer.